
Very often, when speaking with my patients, I realize how important it is to arrive on the day of breast augmentation with all the information clearly in mind.
This will allow you to face the surgery with serenity and with the knowledge that you have made the best choice.
Breast augmentation surgery consists of giving volume to the breasts thanks to the use of breast implants.

But what are the most important aspects of the entire breast augmentation process?
The crucial aspects of this intervention are:
surgical access: where will the scar be?
surgical plan: Where will the prosthesis be placed?
breast implants: What types of prostheses are there?
In this article I will focus on the first two points, but you can delve deeper into the topic of breast implants in a dedicated post.
Surgical accesses
Surgical access refers to the point where the surgeon will make the skin incisions and from where the entire operation will be performed. In practical terms, this is reflected in the location of the surgical scar.
The most commonly performed techniques involve positioning the scar at the level of the mammary fold (i.e., the natural crease at the base of the breast) or at the lower edge of the areola. More rarely, it can be at the level of the axillary fold.
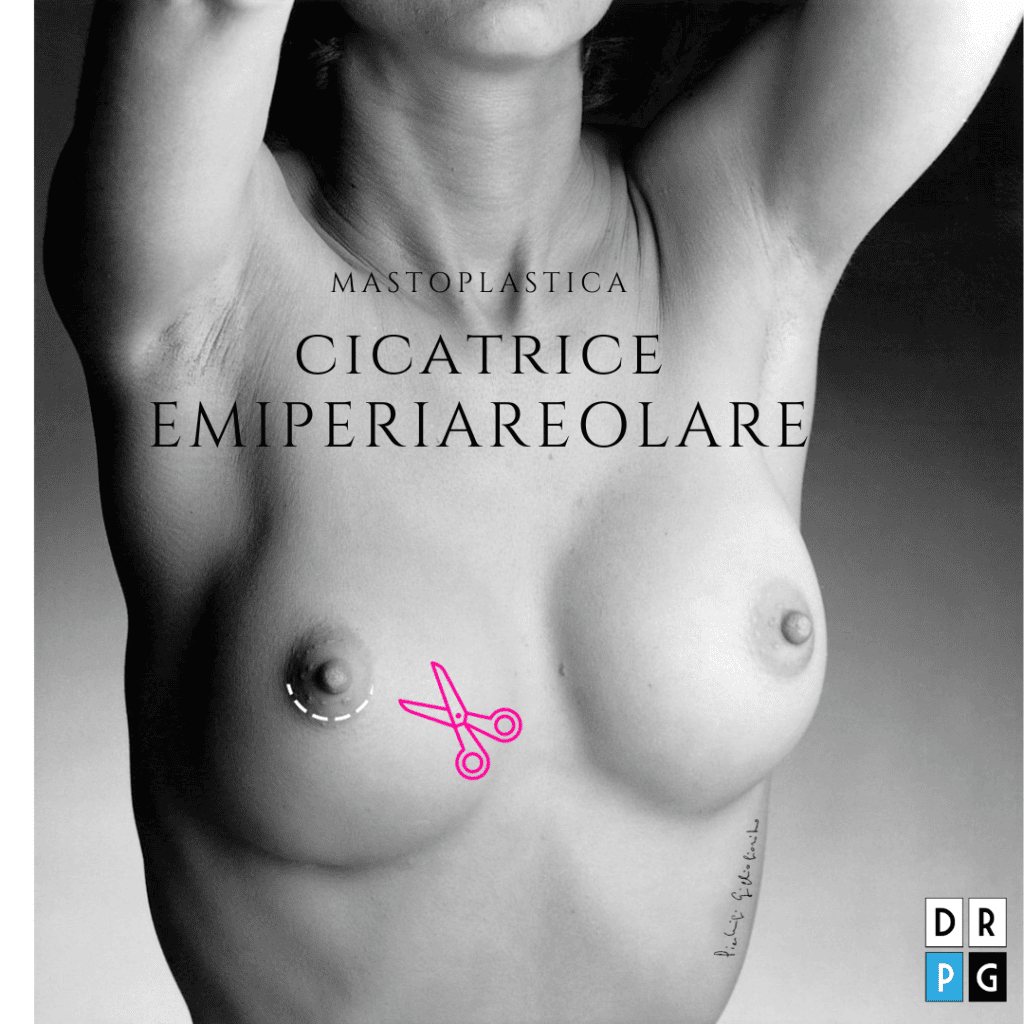
In this case, the scar falls to the lower edge of the areola and takes on the appearance of a small crescent.
The main advantage is that this way the field of vision is wider and the mammary fold, the supporting structure of the entire breast, is not obscured in any way.
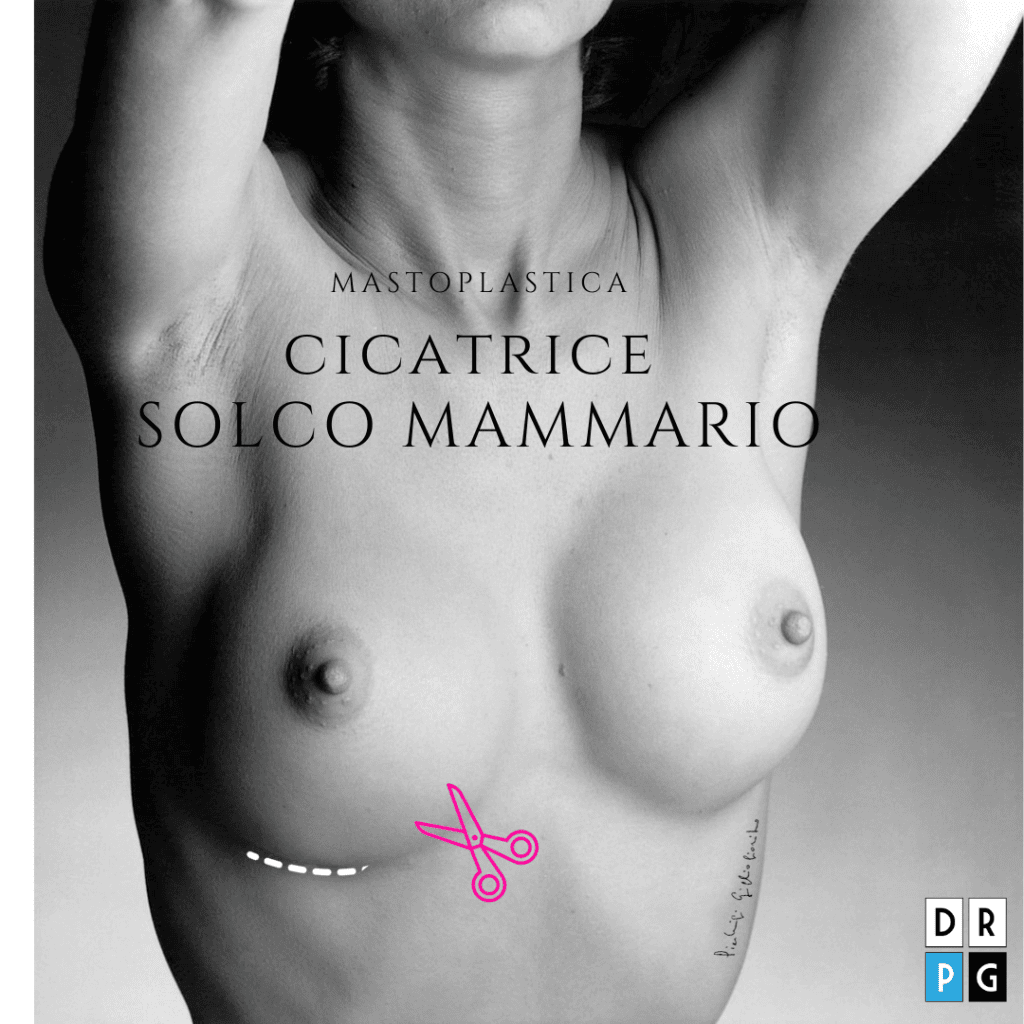
In this case the scar falls at the level of the mammary fold, or the natural fold on which the breast rests.
The main advantage is that the access allows direct access to the pectoral muscle without having to pass through the mammary gland.
The choice of where to position the scar can depend on various factors.
scar:
The position of the scar has no real effect on the success of the operation.
Generally, when the patient is standing and topless, the small scar along the breast fold is almost completely hidden by the breast, while the areolar scar ends in a shadowy area between the darker areola and the lighter breast skin, remaining equally barely visible. Even with very small swimsuits or bras, any potential scars are fairly well hidden and will remain covered.
I personally perform both techniques, although I tend to prefer localized access at the level of the mammary fold, leaving the periareolar approach to cases where there is asymmetry of the areolae or where it is necessary to simultaneously lift the nipple-areola complex, which may have sagged due to pregnancy, breastfeeding, or general weight loss and require a breast lift. This specific type of procedure is called mastopexy, and we will discuss it in a separate article.
Surgical plan
The second aspect to consider during breast augmentation is the surgical plan, or where the system is positioned.
From an anatomical point of view and simplifying the concept considerably, we can imagine the breast as a structure made up of several layers:
– skin and nipple-areola complex (outermost floor)
– adipose tissue (fat) and the mammary gland (intermediate floor)
– pectoralis major muscle (innermost floor)
floor:
Your prosthesis can be placed in front (retroglandular technique) or behind the muscle (retromuscular technique).
The breast prosthesis can therefore be inserted using two techniques:
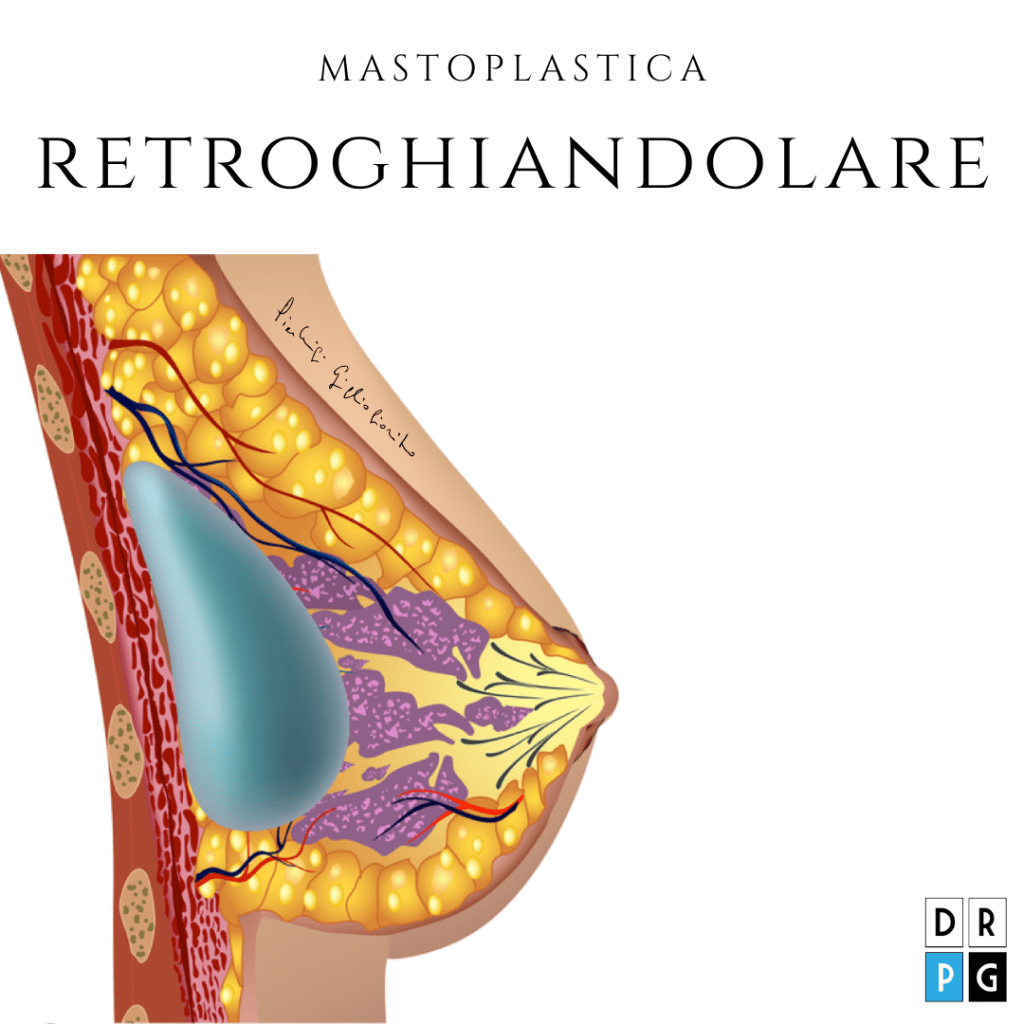
In the subglandular technique, the prosthesis is more superficial, that is, between the mammary gland and the pectoral muscle.
I PRO They are easy to perform, require less time to complete the procedure, and have a much more natural appearance since the prosthesis tends to follow the movements of the breast.
I AGAINST they are a greater risk of capsular contracture and an unnatural appearance on small breasts as the coverage by the gland is less.
This technique involves positioning it underneath the pectoralis major muscle.
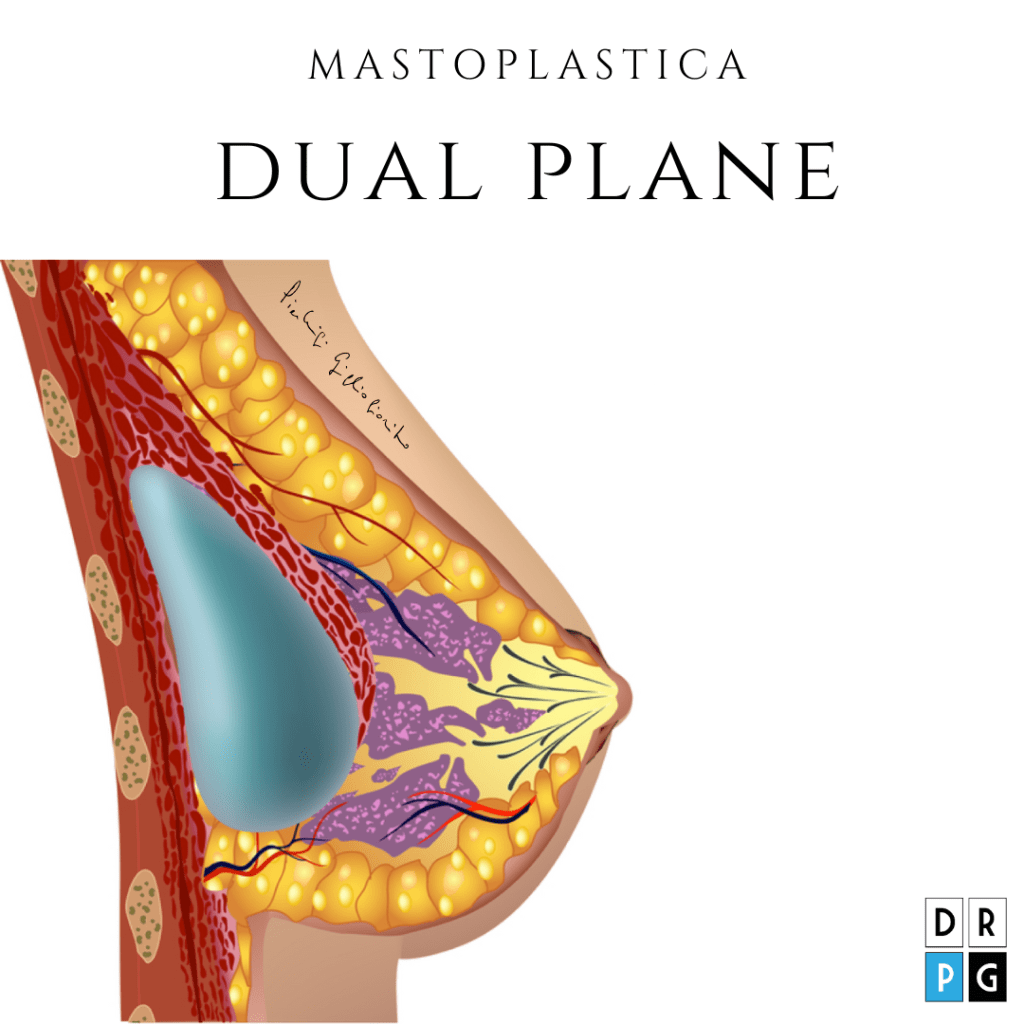
In recent years the technique has gained ground DUAL PLANE in which the prosthesis is covered by muscle in the upper part (from the nipple up) and is subglandular in the lower part (from the nipple down).
I PRO They have a very natural appearance even in patients with little glandular tissue and small breasts to begin with; they reduce the risk of capsular contracture and provide a very natural appearance of the décolleté as it is covered by muscle.
I AGAINST are greater difficulty in execution, a longer duration of the operation and greater post-operative pain related to the muscle incisions.
In conclusion, a question arises spontaneously. Is there a perfect technique? Which one is best for me?
The answer is very simple. There is no perfect prosthesis, just as there is no perfect technique.
There's a technique that's best suited to a particular patient. And all of this must be clarified during the preparatory visits.